Description
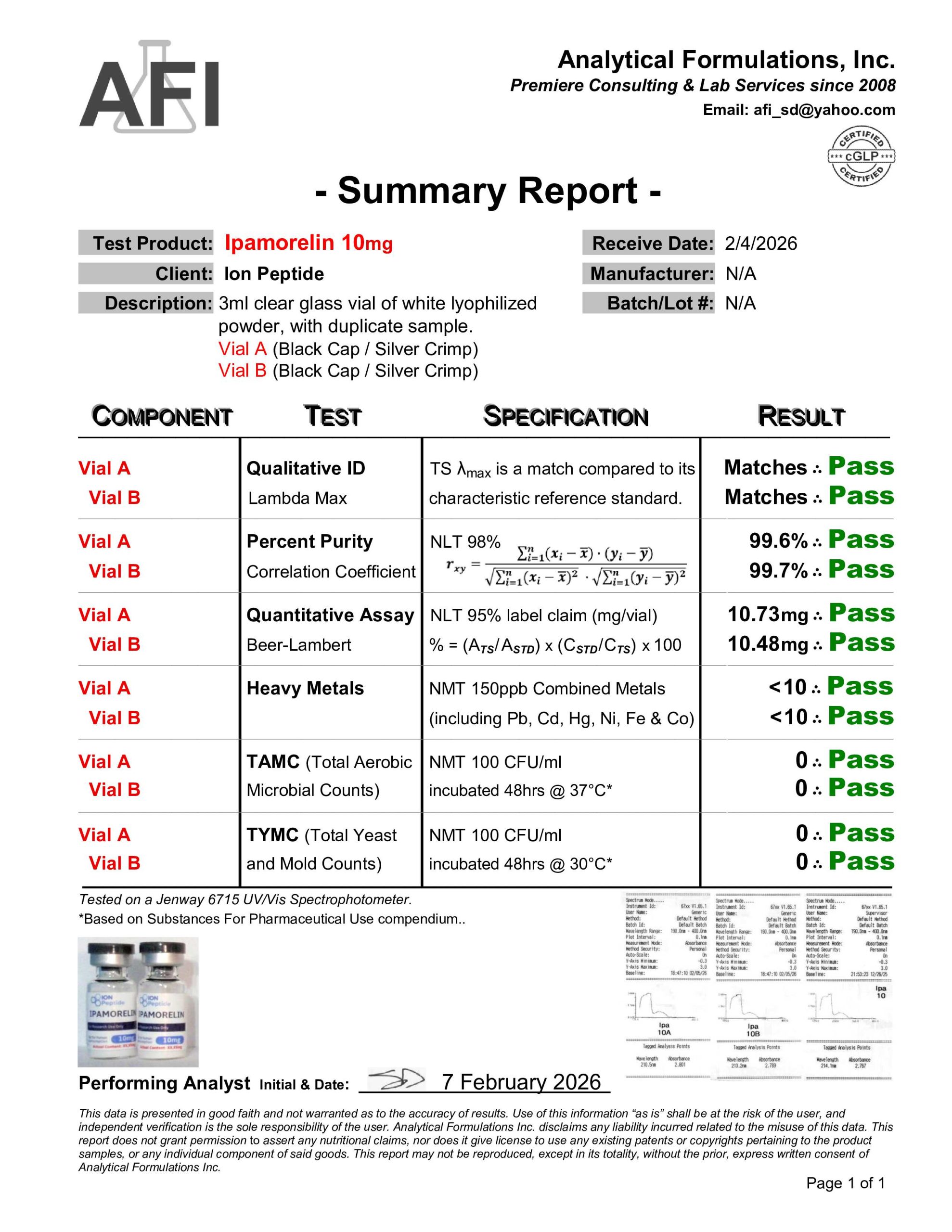
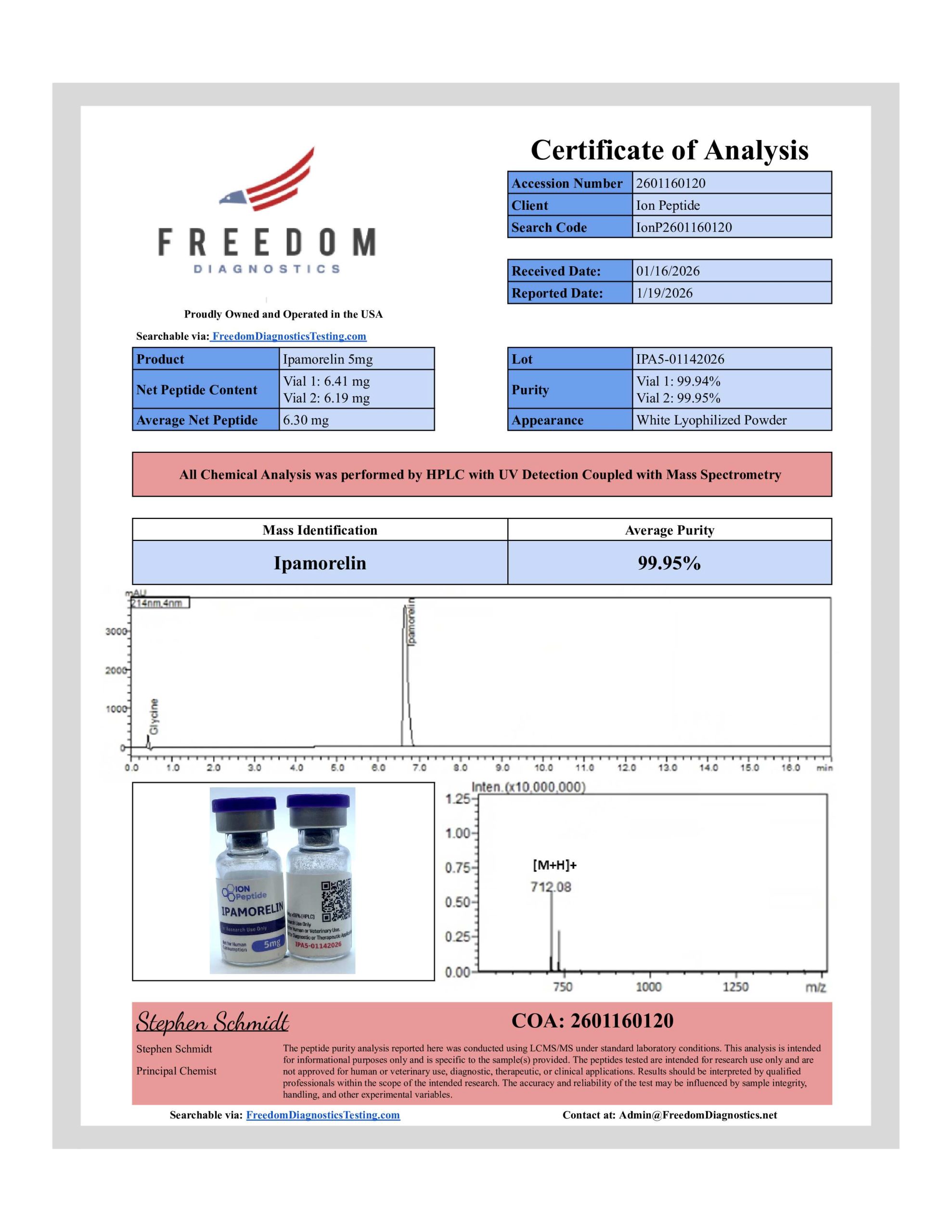
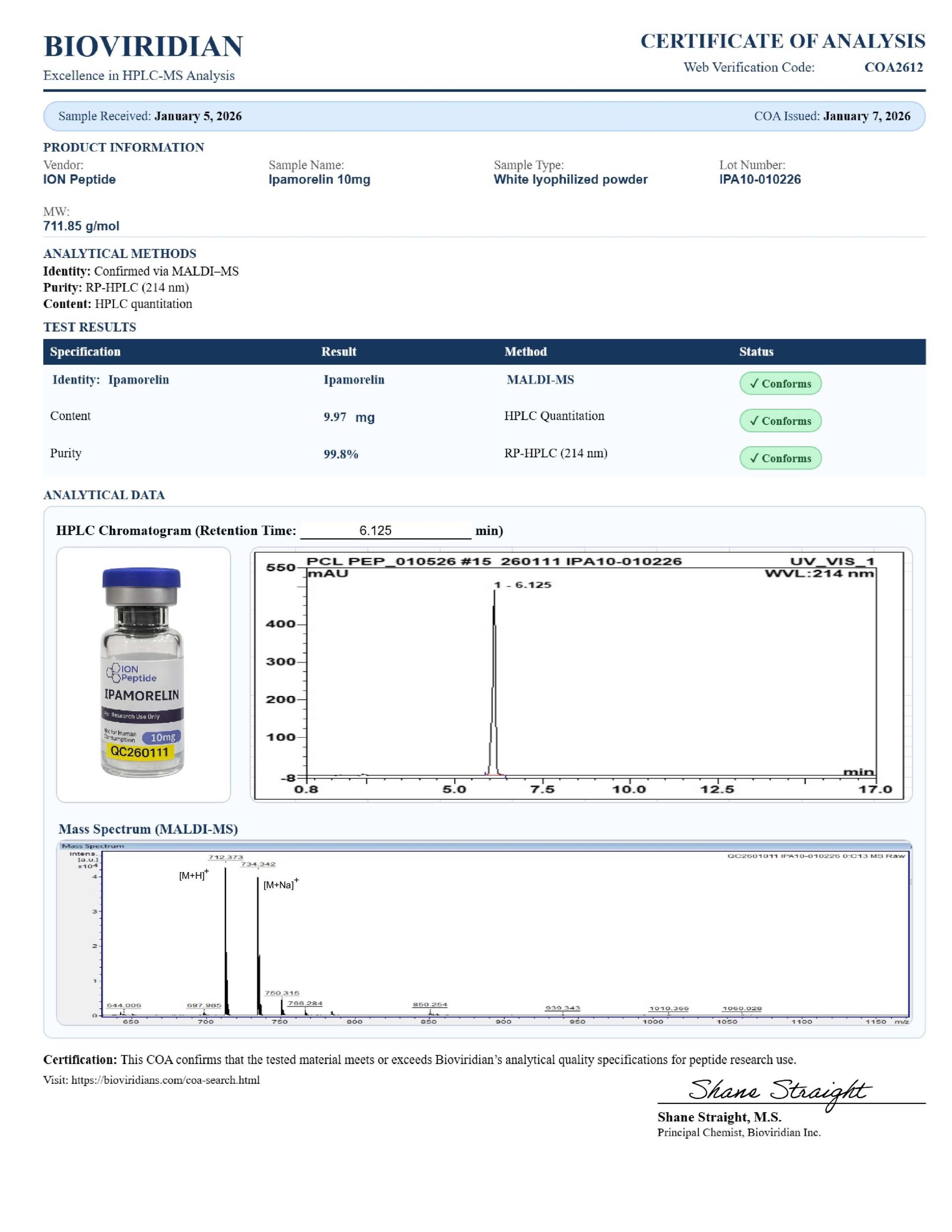
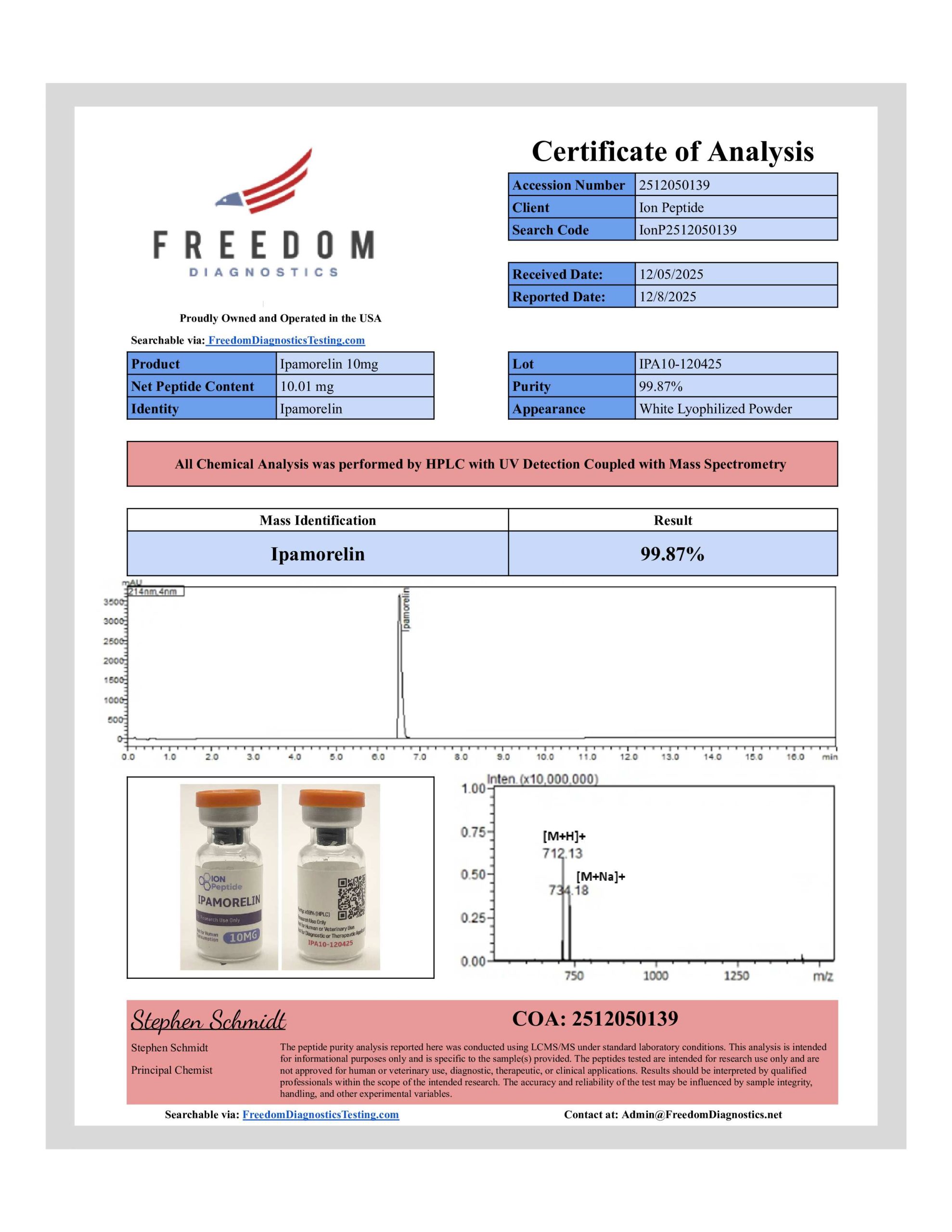
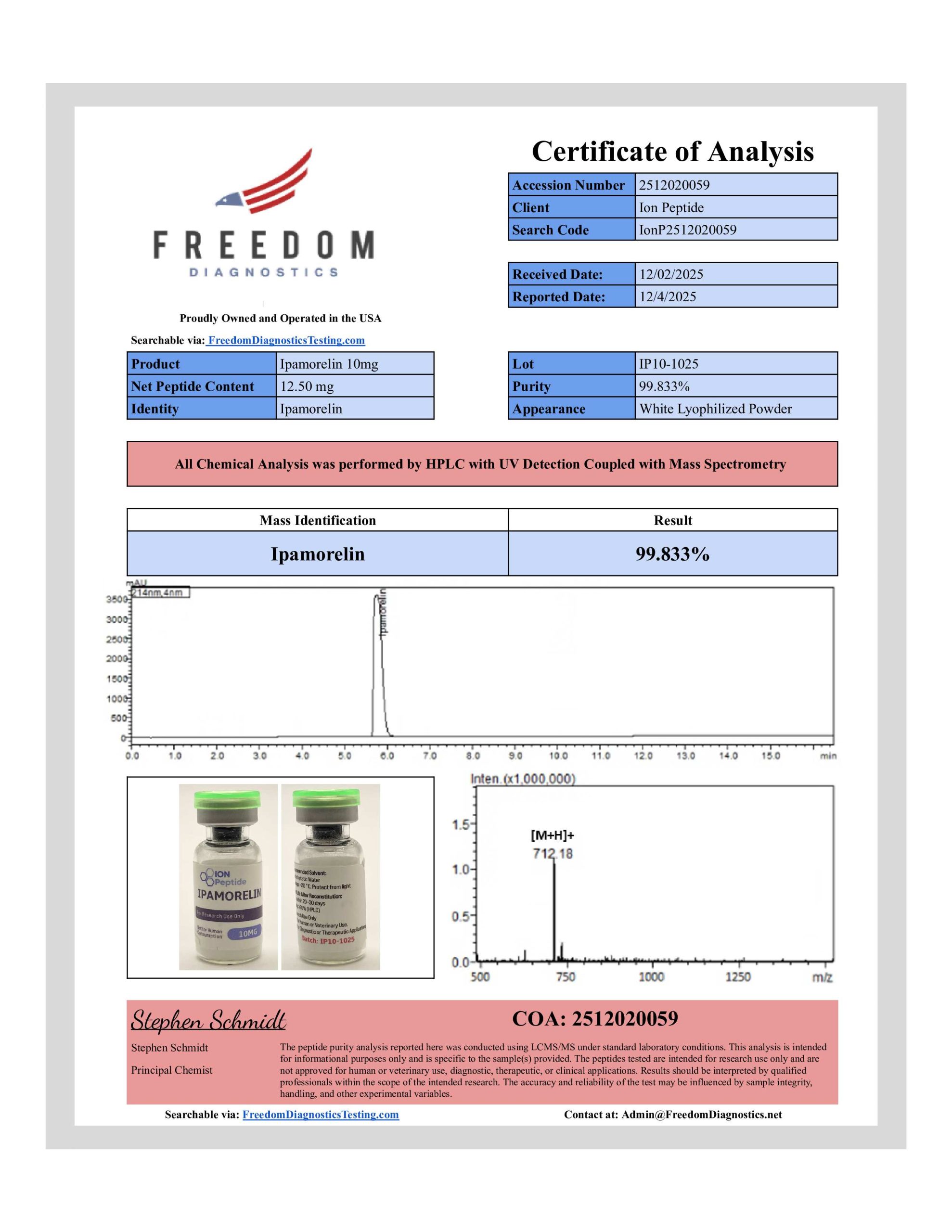
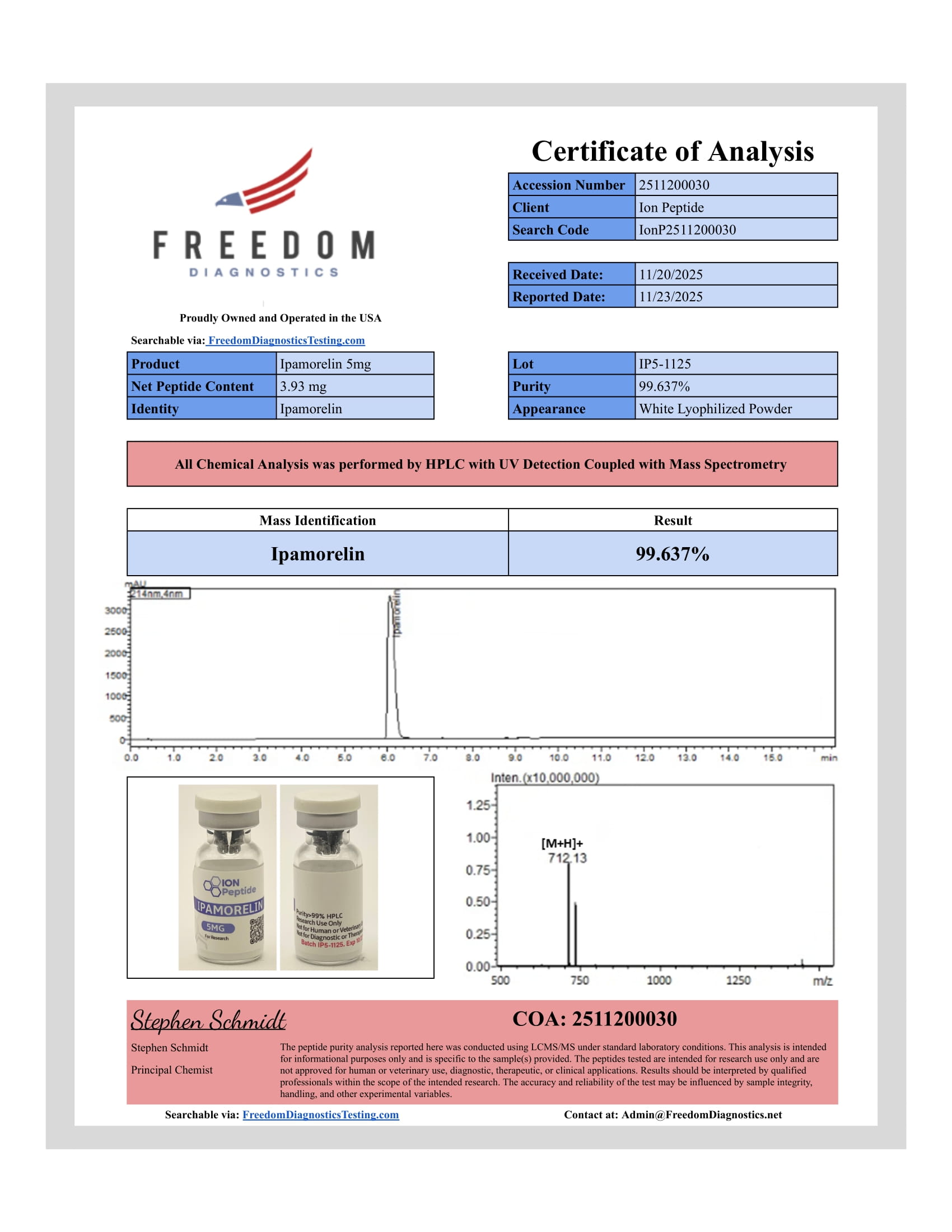
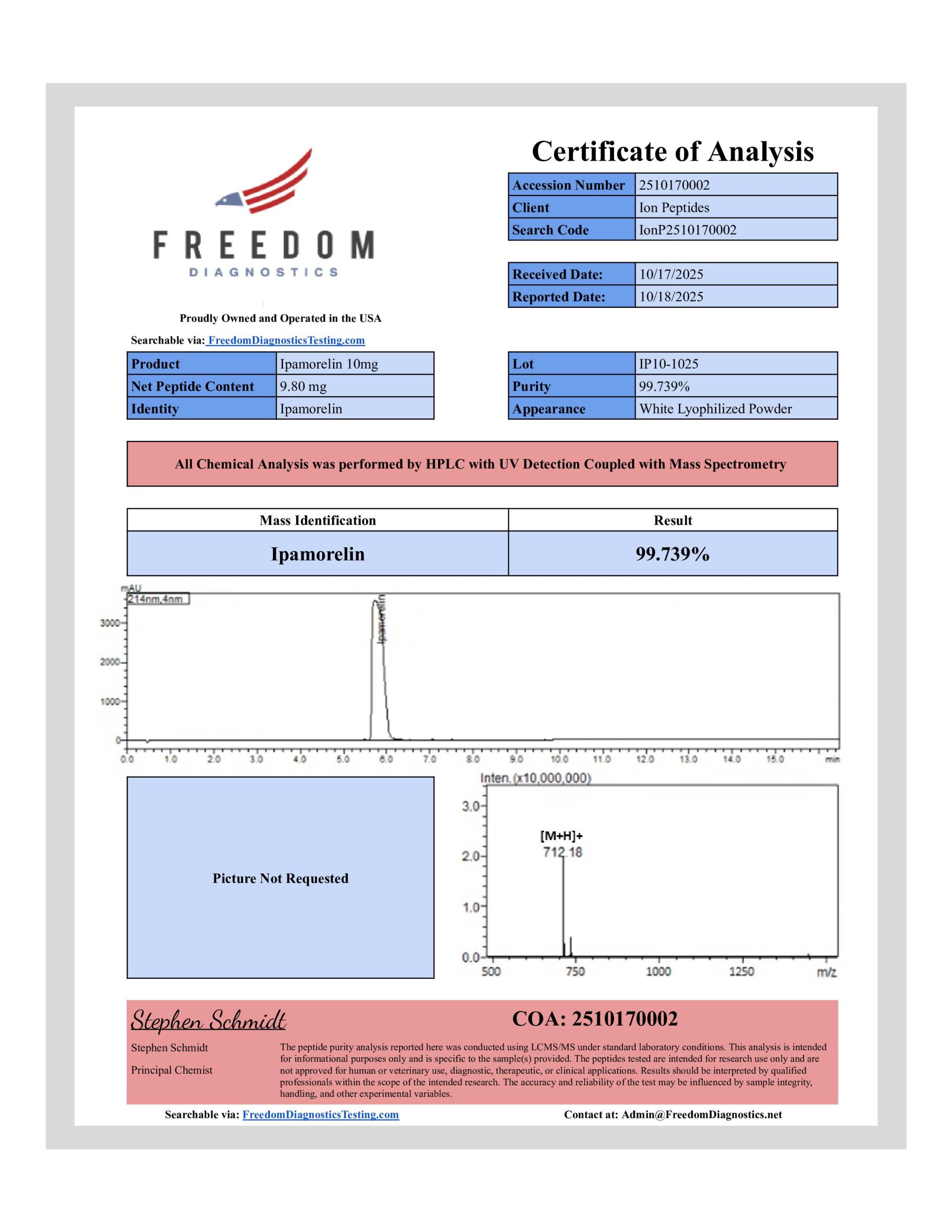
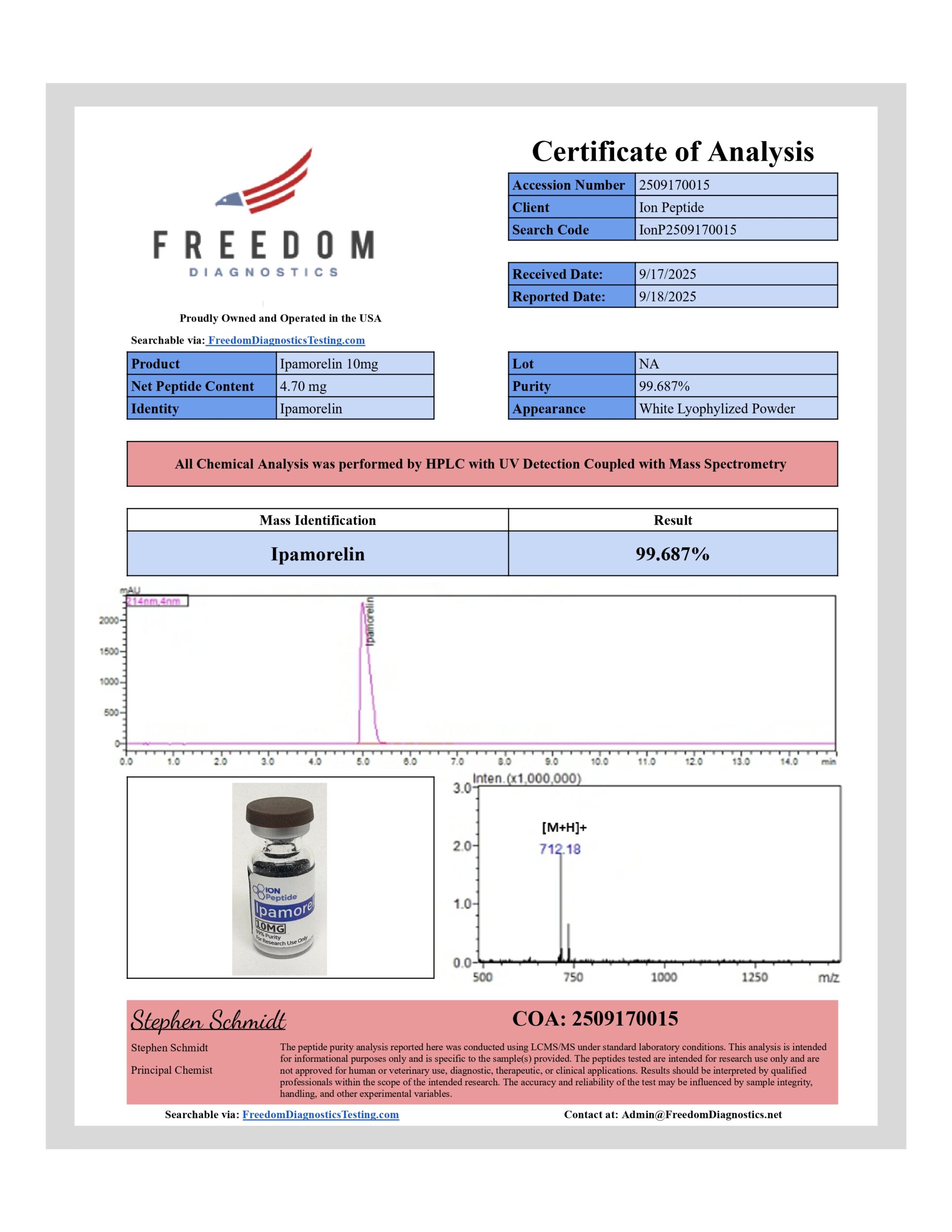
Ipamorelin Peptide
Research-Grade GHRP Analogue
Tagline: Selective GH Secretagogue
Product Description
Ipamorelin is a highly selective growth hormone secretagogue (GHRP) that stimulates GH release via activation of ghrelin (GHS-R1a) receptors. Unlike earlier GHRPs (e.g., GHRP-6), Ipamorelin has minimal impact on cortisol or prolactin levels, making it a more targeted research tool.
Researchers use Ipamorelin Peptide in preclinical models to study pituitary GH release, IGF-1 production, muscle growth pathways, fat metabolism, and tissue repair mechanisms. Its clean receptor profile and short half-life make it ideal for pulsatile GH secretion research.
For Laboratory and Scientific Research Use Only. Not for Human Consumption.
Why Researchers Choose Ipamorelin Peptide
-
Highly Selective: Minimal effect on ACTH, cortisol, and prolactin.
-
Potent GH Release: Strong activation of GH pulses in animal models.
-
Favorable Safety Profile: Reduced off-target endocrine effects compared to GHRP-6 or Hexarelin.
-
Short-Acting: Allows study of physiological pulsatile GH release.
-
Batch Verified: Each lot tested for purity, identity, and potency.
Important Note
For laboratory and scientific research only. Not for human consumption, veterinary use, or diagnostic purposes.